CLEAR Study: Sustained Superiority With Secukinumab Versus Ustekinumab
A comparison of two biologics has shown that secukinumab was more effective than ustekinumab, providing greater and sustained skin clearance at week 52 in patients with moderate-to-severe psoriasis. The head-to-head comparison in the CLEAR study [NCT02074982] was reported by Diamant Thaci, MD, University of Lubeck, Germany, at AAD 2016.
The double-blind study randomized patients to the interleukin (IL)-17A inhibitor secukinumab 300 mg subcutaneously or the IL-12/23 inhibitor ustekinumab 45 mg (patients ≤100 kg at baseline) or 90 mg (patients >100 kg) subcutaneously. Secukinumab was administered at baseline, Weeks 1, 2, and 3, and then every 4 weeks from Weeks 4 to 48, while ustekinumab was administered according to its suggested dosing schedule.
For study enrollment, patients were required to have a Psoriasis Area and Severity Index (PASI) score ≥12, an Investigator’s Global Assessment (IGA) 2011 modified score ≥3, and ≥10% involvement of their body surface area (BSA). They were also required to have been diagnosed at least 6 months prior to screening and to be inadequately controlled with topical, phototherapy, or systemic treatments. Importantly, they had to be naïve to IL-17A and IL-12/23 inhibitors, including the study drugs.
At baseline, the mean age of the patients was 45 years and 30% were women. There was a slight numerical imbalance in the patients with psoriatic arthritis between the treatment groups.
The primary endpoint of superiority of secukinumab versus ustekinumab for the PASI 90 response at Week 16 was achieved and previously reported [Thaci D et al. J Am Acad Dermatol 2015]. A total of 80.1% of the 334 patients in the secukinumab group had a PASI 90 response, compared with 59.0% of the 335 patients in the ustekinumab group (p<0.0001).
Other notable results at Week 16 were a PASI 100 response in 45% of the secukinumab-treated patients and 29.2% of the ustekinumab-treated patients. At Week 4, a PASI 75 response was achieved in 50% and 21% of the groups, respectively (a secondary endpoint). The IGA modified 2011 0/1 response was observed in 84.3% of the secukinumab-treated and 69.6% of the ustekinumab-treated patients at Week 16.
At Week 52, significantly more secukinumab-treated, compared with ustekinumab-treated, patients had PASI 90, PASI 100 responses, and improvement in the Dermatology Life Quality Index (DLQI) 0/1 responses (Table).
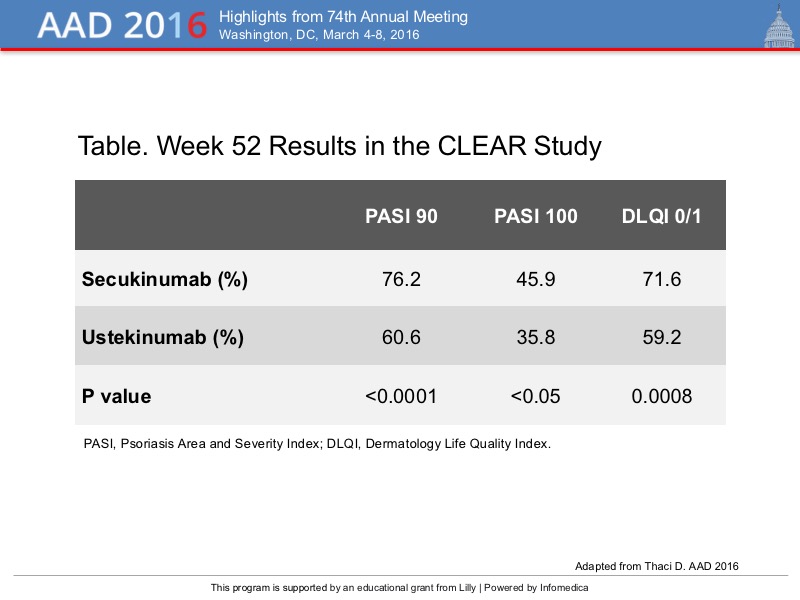{kind=link}
Regarding the DLQI improvement, the significant difference between the treatment groups was observed early (at 4 weeks) and maintained through Week 52.
The safety profile for the two drugs was similar and favorable, with no new unexpected safety signals or toxicities. There was a higher incidence of candida infections with secukinumab than with ustekinumab (6.4% vs. 1.6%), and the infections were characterized as not serious by Dr. Thaci. Tuberculosis, Crohn’s disease, and ulcerative colitis were not observed in any patients in this study.
Overall, the CLEAR study demonstrated that the IL-17A inhibitor secukinumab was superior to the IL-23 inhibitor ustekinumab at Week 16 for the primary endpoint of PASI 90 response, and that this response was sustained to Week 52. Further, early responses (PASI 75) were seen at Week 4 with the IL-17A inhibitor. Nearly half (45.9%) of the secukinumab-treated patients achieved fully clear skin (PASI 100 response) at Week 52. Patient quality of life was improved, as shown by the greater improvement in the DLQI with secukinumab.