Procedural Dermatology: Insights from the Late Breaking Research
Novel agent for the treatment of AGA
Research is moving forward with the novel agent SM04554 for the treatment of androgenetic alopecia (AGA) based on results from a phase 2 study reported at AAD 2016 by Yusuf Yazici, MD, Samumed, LLC, San Diego, California, USA. SM04554 targets the Wnt signaling pathway, which controls stem cell differentiation and is implicated in tissue development and regeneration. In early studies in mice, this topical agent was shown to significantly increase the number of hair follicles.
The multicenter, double-blind, vehicle-controlled trial randomized men with AGA and a Norwood-Hamilton (NH) classification score of 4, 5, 5A, 5V, or 6, to vehicle (n=98), SM04554 0.15% (n=102), or SM04554 0.25% (n=102), for 90 days of treatment. The men were 45 years old, most were white (90%), and about one-third had NH 4 AGA.
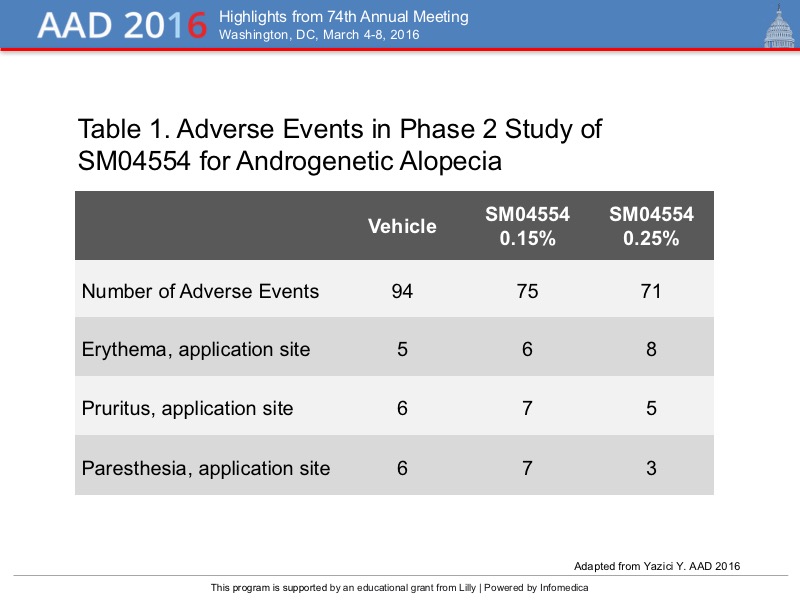
In this study, adverse events (AEs) were defined as all events, including erythema, scaling, pruritus, and burning/stinging, that were increased as identified by the Investigator Scalp Assessment based on a 5-pont scale for each. A total of 137 patients experienced 240 AEs, which are detailed in Table 1. There were no remarkable clinical changes in relation to laboratory parameters, electrocardiograms, and vital signs, stated Dr. Yazici.
{kind=link}
Dose-limiting toxicities (DLTs) were defined as any new onset of a systemic AE ≥ Grade 2 or any new onset local AE ≥ Grade 3, and all were considered to be related to the study medication with subsequent withdrawal from the study. There were no local DLTs reported, and 37 patients reported 44 systemic DLTs (17 with vehicle, 11 with SM04554 0.15%, and 16 with SM04554 0.25%). A small bowel obstruction occurred in one patient treated with vehicle, which was recorded as a serious AE, by the DLT definition. The most common DLTs in the treatment groups were were sinusitis, upper respiratory tract infection, bronchitis, diarrhea, and increase in alanine aminotransferase, but these were limited to 1 or 2 reports.
Regarding efficacy, the intention-to-treat analysis was reported. At 90 days, there was an increase in hair count per 1 cm2 with the 0.15% dose (110.5 vs. 104.9 at baseline), an increase with the 0.25% dose (117.3 vs. 110.8 at baseline), and no change with vehicle (114.3 vs. 115.7). Hair density(µm in 1 cm2) also increased with treatment, from 5656.0at baseline to 5774.5 at 90 days with the 0.15% dose and from 6055.7 to 6277.6 with the 0.25% dose. Hair count and hair density continued to increase through 135 days of follow-up, with a significant difference in the change in mean hair count (p=0.025) and mean hair density (p=0.011).
MFU-V Treatment of Erythematotelangiectatic Rosacea
Microfocused ultrasound with visualization (MFU-V) may be an effective treatment of erythematotelangiectatic rosacea (ER), according to the preliminary results of a study reported by Rosalyn George, MD, Wilmington Dermatology Center, Wilmington, North Carolina, USA.
Focal micro-coagulation zones are created in the skin with MFU-V, leading to thermal-induced tissue contraction and de novo synthesis of collagen. The creation of focal lesions in the dermis and subdermis in the setting of ER is hypothesized to reduce its signs and symptoms, such as erythema.
This multicenter, single-blinded, randomized study used three different treatment depths (4.5 mm, 3.0 mm, and 1.5 mm) and two different densities of MFU-V per treatment square (low density, 15 lines; high density, 30 lines). There were four treatment groups, which received a different combination of number of dual-depth treatments and and density. Group A received 1 dual-depth, low-density treatment; Group B received 2 dual-depth, low-density treatments; Group C received 1 dual-depth, high-density treatment; and Group D received 2 dual-depth, high-density treatments. The second treatment was given 14 days after the first treatment.
Of the 88 patients enrolled to date, 79 were women, and the mean age was 49.8 years (range, 21-65 years). Most patients had a Fitzpatrick score of II (42%) or III (52.3%). The average pain scores were similar across the group, ranging from 3.7 to 6.6.
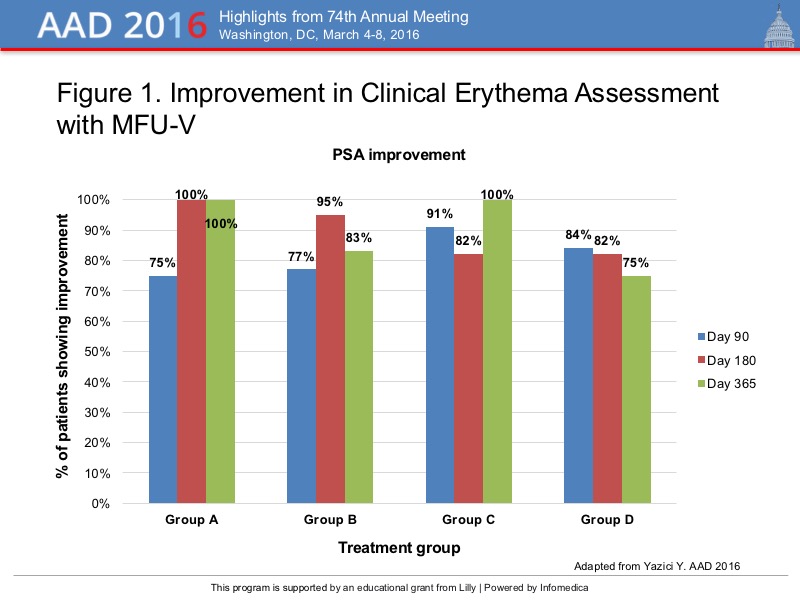
The primary endpoint was the degree of erythema as assessed by the 5-point clinical erythema assessment (CEA) scale at 90 days compared with baseline, with success defined as an improvement of 1 grade in the CEA scale.In this interim analysis, 84 patients had been followed for 90 days, 67 patients for 180 days, and 19 patients for 365 days. The improvement in CEA is shown in Figure 1, with greater levels of improvement with high-density treatment.
{kind=link}
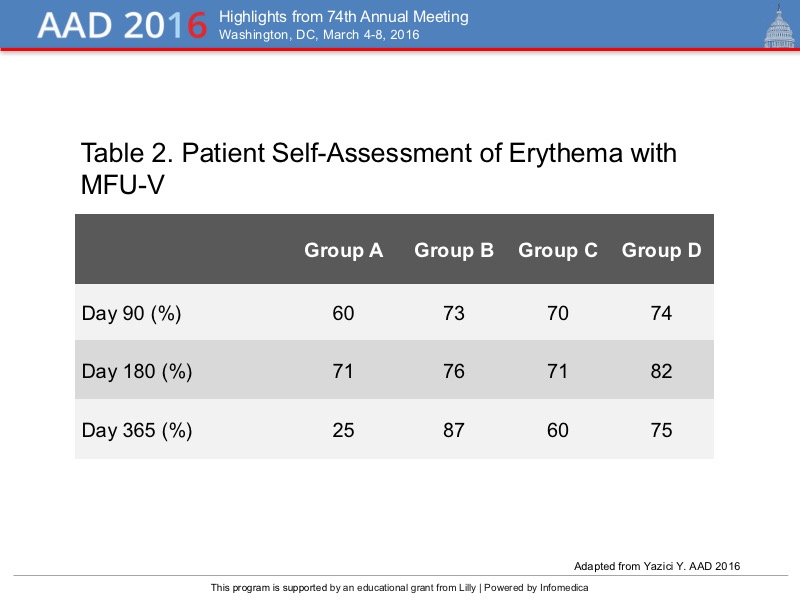
The proportion of patients reporting improvement in the secondary endpoint of self-assessment of erythema (PSAE) is detailed in Table 2. Similar improvement was seen for the secondary endpoint of improvement in colorimeter from baseline.
{kind=link}
No serious adverse events were observed. Bruising was reported by 44%, soreness and tenderness by 43%, paresthesia by 10%, raised area of edema by 17%, and erythema by 35%, but all cases were resolved within 2 weeks.
High-density MFU-V was more effective than low-density MFU-V or superficial treatments in this study of patients with erythematotelangiectatic rosacea. Follow-up is ongoing.