A Revolution in the Treatment of Psoriasis: A Review of New and Emerging Therapies
New treatments that are emerging or have been approved recently for the treatment of psoriasis are bringing unprecedented levels of clearance and hope to patients. Although none of the new treatments cure psoriasis, the level of clearance achieved with the monoclonal antibodies, including Psoriasis Area and Severity Index (PASI) 100 scores in notable proportions of patients, is improving quality of life.
The lack of effective treatment had led many patients with psoriasis to give up on seeking care, but with the availability of these new treatments, they will be returning, said Kenneth B. Gordon, MD, Northwestern University, Chicago, Illinois, USA, in the Hot Topics session. Medical dermatologists must learn how to use these new treatments, including selecting the right biologic for the right patient,
Key mediators of psoriasis are shown in Figure 1. Among the targeted approaches to treat psoriasis is blockade of interleukin (IL)-17A, IL-17F, and IL-17R. Drugs that block IL-17 have been shown to provide an early benefit, at Week 1 in about 30% of patients, and to be associated with high response rates as shown by PASI 75, 90, and 100 scores, that are durable out to 1 and 2 years. In reviewing data with this class of drugs, Mark Lebwohl, MD, Mt. Sinai School of Medicine, New York, NY, USA, noted that an additional advantage is that fewer side effects are anticipated with such drugs, because only a small portion of the immune system is blocked.
{kind=link}
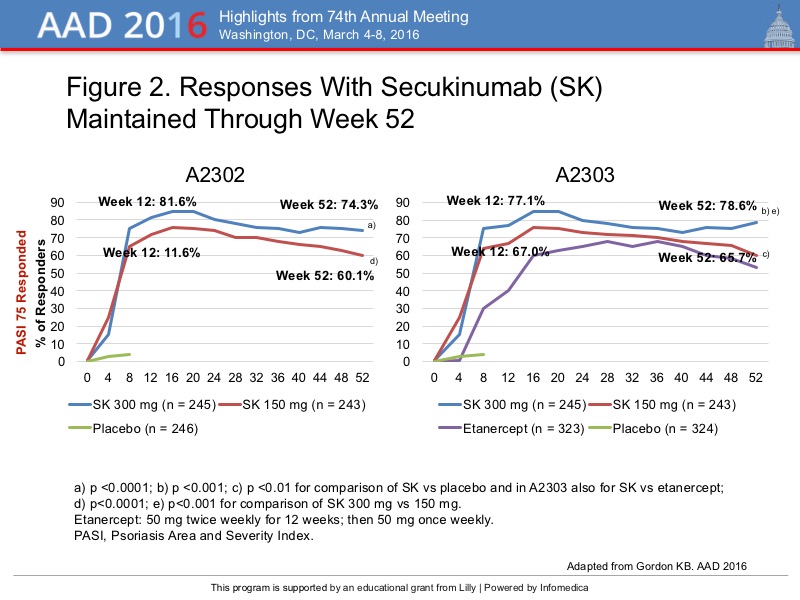
In the pivotal trial of the IL-17A blocker secukinumab, called ERASURE, the 300 mg and 150 mg doses were more effective than placebo at Week 12, with PASI 75 responses of 81.6%, 77.1%, and nearly zero, respectively, in patients with moderate-to-severe psoriasis. These responses were maintained at Week 16 (86.1% and 77.4%) and through Week 52 (Figure 2). In the pivotal FIXTURE trial, both doses of secukinumab were more effective than the tumor necrosis factor (TNF) inhibitor etanercept, with better PASI responses (77.1%, 67.0%, and nearly 60%, respectively) at Week 12, and the responses were maintained to Week 52. Further study showed the response durable to Week 104. Notably, the patients who relapsed on placebo, responded to treatment with secukinumab, with 94.8% recapturing a PASI 75 response, 70.3% with PASI 90 response, and 38.4% with a PASI 100 response at Week 12.
{kind=link}
In UNCOVER-1, the pivotal study of the IL-17A inhibitor ixekizumab in patients with moderate-to-severe psoriasis, PASI 75 responses was achieved in 89.1% with the every-2 week dosing and 82.6% with the every 4-week dosing, compared with 3.9% with placebo (p<0.001). At Week 1, about 30% of patients has a PASI 75 response and about 50% at Week 4. The Week 12 results are shown in Figure 3. About one-third of patients achieved a PASI 100 response with ixekizumab, and a similar proportion achieved static Physician’s Global Assessment scores of 0 (Figure 3).
{kind=link}
Brodalumab, a blocker of IL-17R, was associated with an 85.1% response rate for PASI 75 a Week 12 with the 210 mg every 2-week dose, compared with 69.2% with ustekinumab, in the AMAGINE-3 study. The PASI 90 and PASI 100 response rates were 68.8% and 36.7% with brodalumab, versus 47.6% and 18.5%, with ustekinumab. These PASI responses were maintained through Week 144.
Blockers of IL-23 are also showing impressive rates of clearance. The investigational BI655066 drug was associated with PASI 75 rates in the 90-100% range, PASI 90 rates >90%, and PASI 100 >60%. With a single subcutaneous injection of this drug, 6 of 9 (66%) of patients achieved and maintained a PASI 100 response for 41-66 weeks.
Similarly high response rates were seen with tildrakizumab, an IL-23p19 blocker, at doses of 100-200 mg, the PASI 75 responses were 90-100% through Week 52. In the X-PLORE study, guselkumab was significantly better than adalimumab and placebo, with PASI 75 responses in the 70-80% range.
The TNF-blocker certolizumab, approved for psoriatic arthritis and Crohn’s disease, given at 200 mg every other week produced a PASI 85 response in 74.6% of patients and at the 400 mg dose every week the rates were 82.8%, in a phase 2, randomized, placebo-controlled trial. In RAPID-PsA, a phase 3, double-blind, placebo-controlled, randomized study in patients with psoriatic arthritis treated with certolizumab, the primary endpoint of American College of Rheumatology (ACR) 20 score was achieved in 68.0% of patients with the 200 mg dose and 51.9% with the 400 mg dose, and maintained to 96 weeks in the open-label extension.
The new selective inhibitor of phosphodiesterase 4 (PDE-4), apremilast, produced PASI 75 responses in 33.1% of patients in the pivotal ESTEEM 1 study. Although the response with apremilast is more modest, Dr. Lebwohl noted that it has the advantage of being an oral, rather than injectable, drug. Also, it is the only drug for treating psoriasis that does not require monitoring laboratory values. The side effect profile is good, and is mainly limited to diarrhea and nausea, although the weight loss associated with the drug is about 5% of body weight. In the patients who respond to apremilast, the response tends to be durable, stated Dr. Gordon.
A JAK inhibitor, tofacitinib, is anticipated to be approved in the United States for the treatment of psoriatic arthritis. In a phase 3, placebo- and active-controlled trial, tofacitinib was significantly better than placebo, and was slightly more effective than etanercept. At Week 12, the PASI 75 and 90 responses with tofacitinib 10 mg twice daily, were 63.6% and 36.1%, and with the etanercept they were 58.8% and 32.2%. At the 5 mg dose of tofacitinib, the PASI 75 and 90 responses were 39.5% and 21.0%, which Dr. Lebwohl noted were similar to those achieved with apremilast.
A boron-based PDE-4 inhibitor, crisaborole, has the advantage of being a nonsteroidal agent. In a phase 2a study, 40% of patients had a ≥2-grade improvement in skin clearance, using the Overall Target Plaque Psoriasis Scale. Read about the phase 3 study results with crisaborolein atopic dermatitis in the article titled, Novel PDE-4 Inhibitor Safe, Effective in Mild-to-Moderate Atopic Dermatitis, in our AAD 2016 coverage.