Cardiovascular Event Reduction With TNF-Inhibitors in Patients with Psoriasis
The inflammation resulting from the increased immune activity in psoriasis also increases the risk of cardiovascular (CV) disease and events [Wang Y et al. J Invest Dermatol 2012; Kimball AB et al. Am J Med 2010]. Jashin J. Wu, MD, Kaiser Permanente Los Angeles Medical Center, Los Angeles, California, USA, presented the results of two studies that demonstrated reductions in CV events with a tumor necrosis factor inhibitor (TNFi) in two large cohort of patients, compared with phototherapy, suggesting that treatment that better controls inflammation may reduce CV risk.
Previous work by this research group showed that a TNFi was associated with lower rates of myocardial infarction (MI) compared with phototherapy or topical agents [Wu JJ et al. Arch Dermatol 2012].
One of the presented studies was a retrospective analysis of a large US commercial claims database and included 11,410 patients with psoriasis treated with a TNFi and 12,433 patients with psoriasis treated with phototherapy who were enrolled in a health insurance plan for at least 6 months before and 1 month after the index date. Patients who had been treated with biologics or phototherapy prior to the index date were excluded. The study period was January 2000 to September 2014.
The mean age of the patients treated with a TNFi was 44.9 years and 48.8 years for phototherapy, and 45.9% and 52.0% were women in the two cohorts, respectively. The median follow-up of treatment was 39.9 months and 28.6 months in the TNFi and phototherapy cohort, respectively.
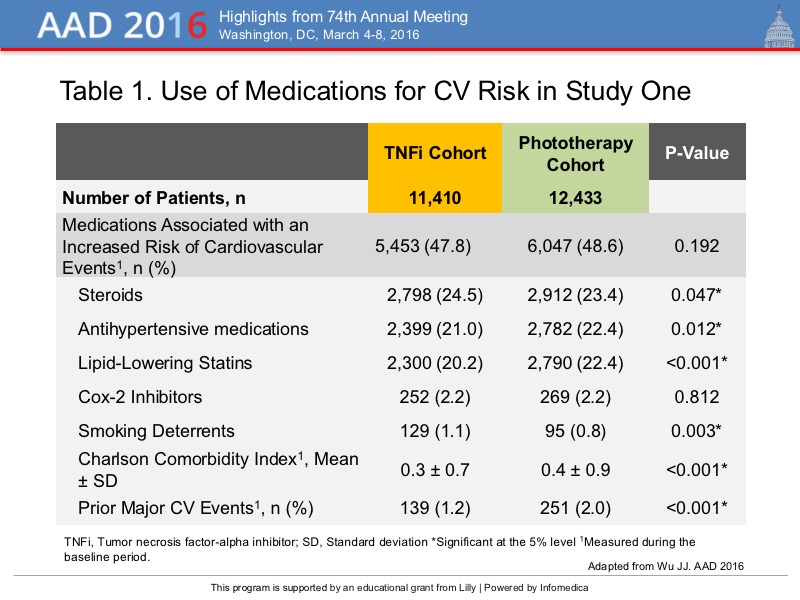
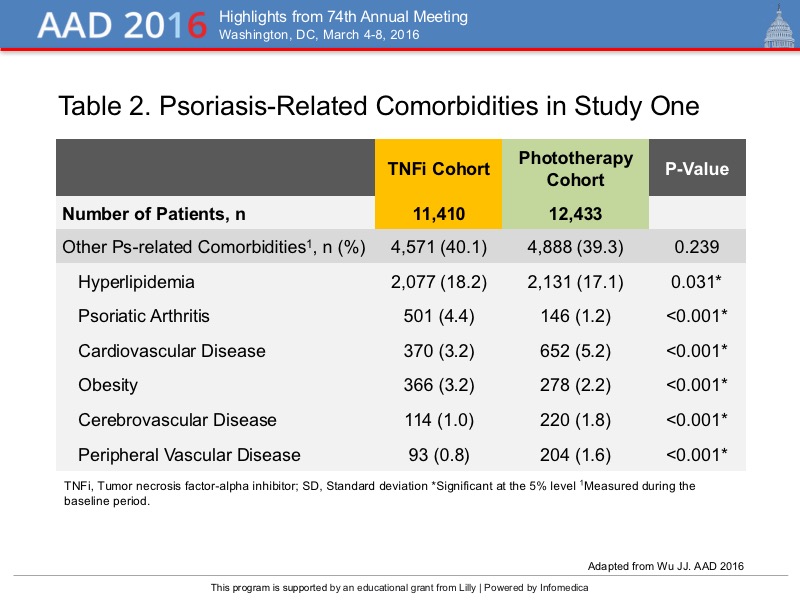
Of the patients treated with a TNFi, 43.4% received adalimumab, 55.6% etanercept, and 0.9% infliximab. Broadband ultraviolet B phototherapy was used in 91% of patients. Medications prescribed for these patients that are associated with an increased risk of CV events are detailed in Table 1 and psoriasis-related comorbidities are detailed in Table 2.
{kind=link}
{kind=link}
For the outcome of the time to the first major CV event, defined as an MI, stroke or transischemic attack, and unstable angina that led to hospitalization, there was a significantly lower rate in the TNFi cohort at 6, 12 and 24 months (0.4%, 0.8%, and 1.4%; p<0.05), compared with the phototherapy cohort (0.7%, 1.3%, and 2.7%). According the Kaplan Meier estimates, a difference was seen between the cohorts at 4 months and continued throughout the study period.
Adjustment for confounders revealed there was a significantly lower risk for a major CV event in the TNFi cohort (hazard ratio, 0.77; p=0.46). Overall during the study period, 106 events occurred in the TNFi cohort and 171 in the phototherapy cohort. A cumulative benefit from TNFi treatment for CV events was suggested by the progressively greater reduction in the hazard ratio over the course of the study, which was 11.2% at 6 months, 21.1% at 12 months, and 29.9% at 24 months.
In the second study, a retrospective cohort analysis using the Kaiser Permanente Southern California health plan database, the risk of major adverse CV events was evaluated in 1,605 patients with psoriasis receiving an TNFi for at least 2 months, 3,339 who were TNFi naïve and received oral agents or phototherapy (oral/photo cohort), and 10,350 who were not treated with TNFi, other systemic treatments or phototherapy (topical cohort). The median duration of follow-up for these three groups, respectively, were 9.5 years, 8.5 years, and 8.1 years.
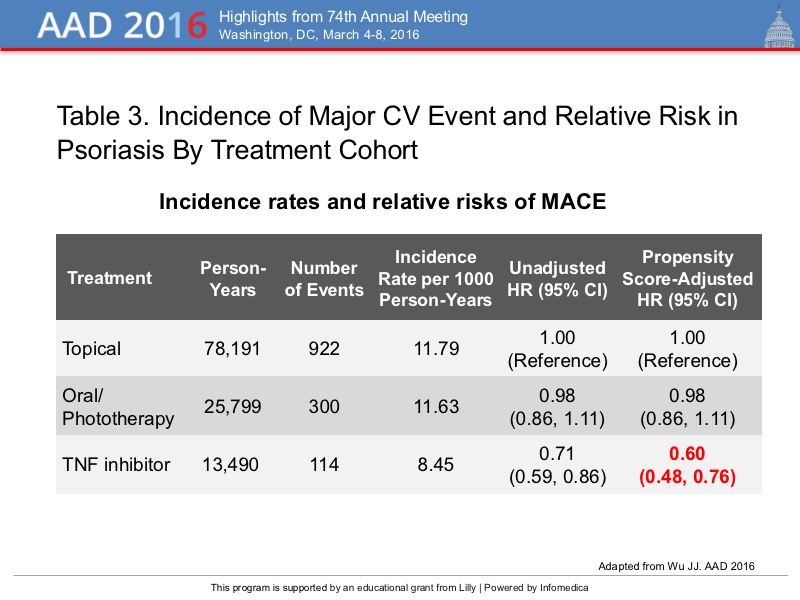
The incidence of a major adverse CV event, defined as an MI, stroke, and CV death in these patients with psoriasis is detailed in Table 3. The incidence was lower with TNFi treatment. After adjusting for risk factors for a major CV event, there was a significantly lower risk of an event in the TNFi cohort compared with the other two cohorts.
{kind=link}
The reductions in the risk for major cardiovascular events, including MI, stroke or transischemic attack, unstable angina, and cardiovascular death, demonstrated in these two large-scale studies with a TNFi, compared with phototherapy or topical therapy, contributes to the evidence of a protective effect of TNFi on cardiovascular outcomes in patients with psoriasis.