IL-17A Inhibition With Ixekizumab Durable in Psoriasis Patients in UNCOVER-3 Study
The durability of the effect of ixekizumab in patients with moderate-to-severe plaque psoriasis was demonstrated with the 60-week results from the phase 3 UNCOVER-3 study, reported at AAD 2016 by Andrew Blauvelt, MD, MBA, Oregon Medical Research Center, Portland, Oregon, USA. The safety and efficacy results at Week 60 with this investigational drug echo those reported at Week 12 [Griffiths CE et al. Lancet 2015].
Ixekizumab is a humanized, high-affinity monoclonal antibody against the proinflammatory cytokine interleukin (IL)-17A. A large body of basic science research supports IL-17A as a critical effector cytokine in psoriasis.
The multicenter, placebo-controlled and active-controlled trial randomized 193 patients to placebo, 382 patients to etanercept 50 mg twice weekly, 386 patients to ixekizumab 80 mg every 4 weeks, and 385 patients to ixekizumab 80 mg every 2 weeks for the induction period. The patients in the ixekizumab groups had an initial starting dose of 160 mg. After the 12-week induction period, all patients entered the open-label treatment phase of the study with ixekizumab 80 mg every 4 weeks.
The study enrolled patients who had been diagnosed with chronic plaque psoriasis at least 6 months prior to screening, and who had, at screening and the baseline visit, involvement of ≥10% of body surface area (BSA) and a psoriasis area and severity index (PASI) score ≥12. The study patients also had at least moderate clinical severity, as measured by a static physician global assessment (sPGA) score ≥3. Previous treatment with etanercept was an exclusion criterion.
At baseline, the patients were 46 years old and about 30% were women. Their mean duration of psoriasis was about 18 years, and about 28% of their BSA was affected by psoriasis. The mean PASI score was 21, Dermatology Life Quality Index (DLQI) was 12, and Itch Numerical Rating Score was about 6.5.
Dr. Blauvelt reported only the analysis of the patients who were treated continuously with only ixekizumab from Week 0 to Week 60, with nonresponder imputation for missing data.
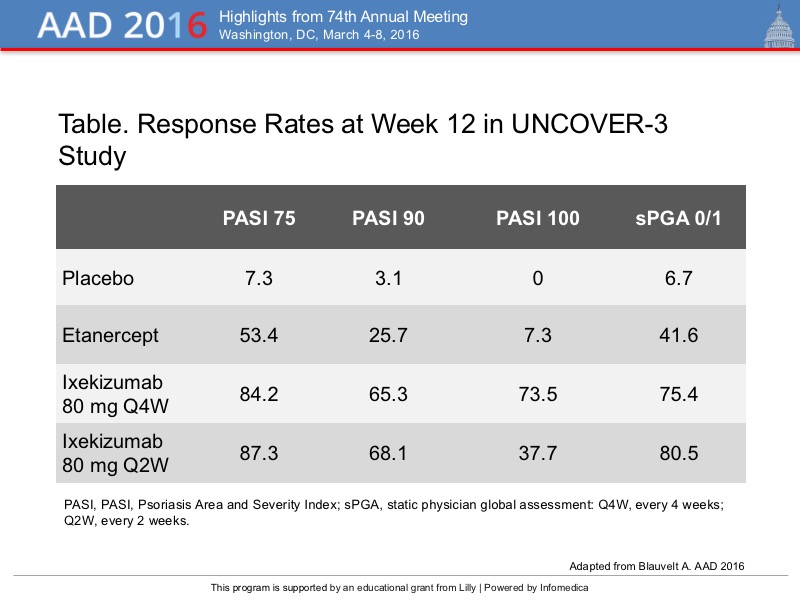
At week 12, after the induction period, ixekizumab was associated with response rates greater than 80% for PASI 75 and 60% for PASI 90, and nearly 40% for PASI 100, compared with placebo and etanercept, and a high rate of sPGA 0/1 responses (Table).
{kind=link}
At Week 60 of the ixekizumab Q4W open label extension, a PASI 75 response was achieved in 79.5% and 83.4% of patients in the ixekizumab Q4W and Q2W induction phase groups. Also in these groups of patients, the rate of a PASI 90 response was 71.0% and 73.2%, respectively, and the rate of a PASI 100 response was 52.1% and 55.3%. The sPGA 0/1 response rate was 72.8% and 74.5%, respectively.
The intention-to-treat analysis of 771 patients revealed response rates of 82%, 72%, and 54% for PASI 75, PASI 90, and PASI 100, respectively, and 74% for sPGA 0/1. These rates of response were also observed in the 722 patients who received at least one dose of ixekizumab during the open-label extension study, with PASI 75, 90, and 100 scores of 87%, 77%, and 57%, respectively, and 79% for sPGA 0/1.
The safety profile ixekizumab during the open label extension was similar to that in the induction phase with no unexpected safety signals through Week 60. The rate of discontinuation because of adverse events was 4.9% with placebo, 6.1% with ixekizumab Q4W/Q4W, and 4.1% for ixekizumab Q2W/Q4W. Treatment-emergent AEs occurred in about 80% of each group, of which 30% were mild and 40% were moderate.
In the UNCOVER-3 study of patients with moderate-to-severe plaque psoriasis, the high level of clinical responses achieved with ixekizumab were maintained to Week 60, and more than half of patients had complete resolution of their psoriasis.